CASE PROTOCOL "ENURESIS"
Greetings, friends.
In my last phase of studies of Behavioral Guidance, I studied in the CIPPSV (Center for Psychiatric, Psychological and Sexological Research of Venezuela) Núcleo Táchira, San Cristóbal, Venezuela; we are asked as part of our training to carry out studies of specific cases related to behavioral problems, feeding, sleep, difficulties to go to the bathroom alone, phobias, hyperactivity, lack of attention and learning difficulties, among others that give origin to the inability to progress and develop comprehensively.
This is how the realization of case protocols are activities carried out with the purpose of gathering the maximum amount of information to be handled, studied and analyzed. These protocols are characterized by providing a set of rules and norms to follow that mark a visible and standard formality within the guidelines of the Institute.
Within these, they can be mentioned: the oriented is identified only with the initials of their first and last names, the parents of the oriented must also be identified in this way, they have a personal data series for a better record, the history of family and personal history, it is necessary to build a Genitogram, which is nothing more than the graph or graphic representation of the genealogy of the oriented.
In particular, I am pleased to present in this post the case study of Enuresis; for a brief description of this behavior alteration.

SOURCE
{kind=link}
Enuresis can be understood as intermittent urinary incontinence that occurs during sleep. This term is also used when there is also diurnal urinary incontinence; then enuresis is nothing more than the repeated emission of urine in bed or clothing, involuntarily or intentionally.
It should be noted that the behavior is clinically significant and manifests with a frequency of 2 times per week for a period of 3 consecutive months. The chronological age, from which it is considered a problem, is five years, in the case of girls and six years in the case of boys, or an equivalent level of development.
Gómez Restrepo, conceptualizes enuresis as "a disorder of the control of sphincters characterized by involuntary urination, repeated, but complete, in a child whose adequate development would allow him to have acquired it, and who does not present a medical illness ...". [1] This conceptualization clarifies that enuresis, rather than a symptom, whether it is isolated or interrelated, is a rather complex clinical appearance, constituted by physical, psychological and environmental elements.
I. IDENTIFICATION
Surnames and names: A.J.G.H.
Date of birth: 10/01/2010
Age: 7 years
Sex: Female
Marital status: Single
Profession: Student
Level of Instruction: 2nd Degree of Basic Education
Religion: Christian Evangelical
Address: Santa Cruz Edo- Zulia
II. REFERENCE
The Mother.
III. DATA SUPPLIED BY:
The information was provided by the mother and the guidance.
IV REASON FOR CONSULTATION
The mother: manifests: "My girl has taken the habit of wetting herself in bed every night whenever dawn I get her clothes and blankets wet with urine. I scold her every time, every morning is a fight, I talk a lot with her and I explain that she is already big for that to happen, I told her to let me know if she is afraid to get up at night to go to the bathroom, I order her to bathe every morning. "
The oriented: says: "before going to bed I go to the bathroom, but I do not understand why my urine comes out. I realize because it makes me very cold and when I check I'm already urinated. "
V. CURRENT PROBLEM
A.J.G.H. female, with 7 years old, 2nd grade student of Primary Education, of thin build, white skin, light brown hair and blue eyes, presents behaviors of enuresis manifested in wetting clothes and bed when sleeping for nights The oriented was taken to a specialist does not present any organic difficulty.
When it starts: About 1 year ago.
How it starts: When you lie on your bed, urinating on the bed and sheets at night or at dawn
Situation in which it occurs: When you sleep at night.
How often: Every night. Always at sleep
What is attributed to him: At the birth of his new sister. When sleeping alone in his bed.
VI. FAMILY AND PERSONAL BACKGROUNDS
Family members:
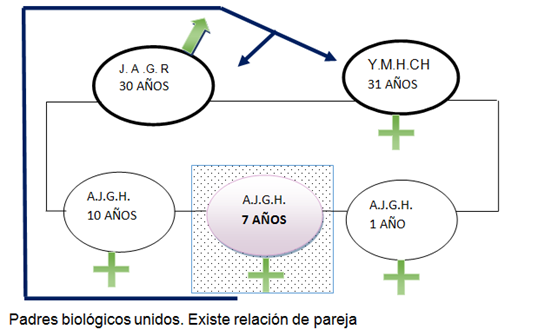
Constitution of the Family: A.J.G.H. belongs to a monogamous family, composed of father, mother, sisters and the oriented
Father: J.A.G.R. 30 years old, with a sturdy frame, white skin, straight brown hair, blue eyes. Cabero
Mother: Y.M.H.CH. 31 years old, robust build, white skin, curly black hair, brown eyes. Executive of the home.
Sister: A.J.G.H. 10 years old, white skin, curly black hair, brown eyes.
Sister: A.J.G.H. of 01 year old, white skin, curly hair of black color, brown eyes.
Relationship intrafamiliares
Father: J.A.G.R. The relationship with the oriented is pleasant and operative there is reciprocal communication with it.
Mother: Y.M.H.CH. His relationship with the oriented is quiet where he shows affection through hugs and affection.
Sister: A.J.G.H. She is affectionate and very attentive to the oriented, they share games, and love is manifested through hugs and kisses.
Sister: A.J.G.H. their relationship is of very little interest, the manifestations of love on the part of the sister-oriented one are very absent.
Communication
Father: The communication with the father is operative, calm and fluid; however for work reasons it occurs very rarely a day.
Mother: Communication is very natural, expressive and colloquial, that is, operative at the time of transmitting ideas, or inconveniences as well as when communicating, joys and surprises.
Sister: The communication with her sister with her older sister is operative, amusing between games and amusements.
Personal:
Since it occupies the family: The oriented is the second of three sisters.
Interpersonal Relations: The relationship between the family is pleasant, and operational, as with their peers and older sister, there is reciprocal communication.
Expression and receptivity of affection: The oriented is affectionate with his family and companions and has received affection from his parents and older sister, but he has trouble expressing affection for his younger sister.
Medical background: The oriented has presented from very small constant flu and allergies.
Oriented health: Due to the flu, refriados and allergies has had some respiratory crises.
VII. GENITOGRAM
VIII. SOCIOECONOMIC CONDITIONS
Father's profession: J.A.G.R. He has 6th grade completed, he works as a caveman in a Refrigerator.
Profession of the mother: Y.M.H.CH the mother is executive of the home.
Family income: Family income depends only on the father with a minimum wage, monthly salary and / or weekly work product of daily work.
Type of house: House with two rooms, 1 bathroom, kitchen, living room, large patio, with good sanitary conditions and with all public services.
Socioeconomic level: According to the socio-economic parameters of the Graffar scale, it is located with a score of 12, finding itself in stratum IV with a low classification.
IX. BIOGRAPHICAL HISTORY:
Psychomotor development: A.J.G.H. was conceived of a pregnancy desired by their parents, was born by cesarean delivery, without any problem, at birth, 3,300 grams and measured 50 cm began crawling 7 months and sat at 8 months, stood in the pen at 9 months, whispered his first words at 9 months, walked to the year and four months and controlled sphincters at 2 years and a half
Socio-affective area: A.J.G.H. she has been a dynamic girl, affectionate with the family especially with her paternal grandparents, classmates and friends, attached to her parents, she has always expressed her feelings in a natural way, at all times she shares with her older sister; However, she shows disinterest and little attachment for her younger sister, without expressing expressions of love towards her.
Student history: A.J.G.H. He started in pre-school when he was 4 years old, he carried out his Initial Education levels normally. Next course the 1st grade at 6 years. Currently finishing the second grade of Primary Education, its academic performance is optimal, however in recent months has shown disinterest.
Sexual History: A.J.G.H. she identifies with her sex, dresses, behaves and plays her own sex.
X. DIAGNOSIS:
A.J.G.H. A female 7-year-old chronological student, in the 2nd grade of Primary Education, presents in her home a non-operative behavior of enuresis manifested in urinating on clothes and bed while she sleeps at night. According to the criterion of the Physiological Model Vs Sociocultural Model, it is a socially rejected non-operative behavior is a physiological behavior because it has no organic problem, socially rejected, motivated by the constant calls for attention made by his mother. According to Approach B, Normality Criteria the behavior is altering the psychological variable, plus this behavior attentive to personal growth. In Focus E, Roles, his role as a person is altered, because the behavior of enuresis seen by others can affect his personality. The girl showed willingness to help her.
XI. BEHAVIORAL ANALYSIS
Physical environment where the problem occurs: Home
Absent Behavior: Sphincter control.
Decreased Behaviors: Affection, communication, high self-esteem
Augmented Behavior: Enuresis (wetting clothes and bed).
Behavior that you want to modify: Enuresis (wetting your clothes and bed).
Define Parameters: Observation, interview and application of registration tables and frequencies were used to study the behavior.
REFERENCES:
[1] GOMEZ RESTREPO, C. (2008), Clinical Psychiatry: diagnosis and
treatment in children, adolescents and adults, Third Edition,
Bogotá: Editorial Medica Internacional.