The Art of the Physical Examination
The physical exam— one of my favorite aspects of medicine. I refer to it as an “art" because someone, or some AI for that matter, could know every medical fact in the world, but could fail to be a good detective. In other words, a doctor not only needs to be smart, but needs to be clever and insightful. No matter how much the world advances in technology, the physical exam will always have its importance. It can save someone from needing an unnecessary amount of radiation if imaging is not necessary. It can alert a physician to something so critical that there is no time for imaging or lab tests. A good physical exam, may lead someone to the operating table before any lab result is analyzed.

While the most important element to diagnosing a patient is the subjective history—that has its flaws as well. A patient may be in pain but unable to describe the condition he is suffering from. Patients may have nonspecific symptoms that are not being described well in words...
Subjective is subjective for a reason. Every patient has a different degree of pain tolerance. A 10/10 in pain for someone having constipation could be a 1/10 pain for someone else. Someone could say, yeah “my tummy hurts pretty bad,” which could mean…"Yeah my appendix has ruptured!" That is when an objective analysis has its importance.
While trusting patients is an important aspect to any doctor-patient relationship, the people who try to take advantage of the system for any reason need to be objectively observed as well. With the increasing addiction to pain medication, people certainly take advantage. There is also psychological problems where people don’t tell the objective truth, when they themselves, don’t even know what is reality. Someone who has a pseudo-seizure, may actually experience a seizure, but it is not organic. Others know they are not having one, but do it to for some unknown benefit—maybe just attention.
Seeing physicians as "detectives in saving lives" is an awesome element to medicine! I am in my last year of medical school, and this is an art that I am only beginning to develop. This is an art where experience makes you the best. IQ and medical knowledge can benefit a patient, but experience in medical situations is what can bring the most importance to a patient. I have learned much of what I need as far as knowledge in medical pathology, but the physical exam/detective skills is something I will always be able to improve upon the most.
Personal Story of Finding an Aortic Aneurysm on just Physical Examination:
I was doing a month of cardiology in July, and I found a big one! One that is written in the textbooks but only if you are looking/thinking will you find it. I saw a patient, complaining of a syncopal (passing out) episode while on the golf course. He was a heavy drinker and likely was experiencing a combination of problems leading to his syncope. On physical exam, the heart, the peripheral cranial nerves, his hydration status, his mental status, and his carotid arteries were all on my mind. These were important things to consider as they all could have lead to his symptoms. However, when admitting a patient to the hospital, everything should be considered…
When I was doing the “abdominal examination", I noticed something subtle. A slight pulsation near the upper-left midline of his abdomen. I felt this pulsation and felt a hard, powerful pulse—his aorta! In skinny people this is not hard to do. I mean, the aorta is a very big artery. However, this male was over-weight and that to me was a factor that made me more concerned. Why was I feeling his aorta through all that adipose (fat tissue)? The answer is…I shouldn’t have if this person did not have pathology.
The first thing that came to mind was that this aorta had widened. The wall of the artery was compromised and thinner to be producing this objective finding. I decided to alert the attending cardiologist that this patient needed an abdominal ultrasound. After his physical examination of the aorta, he agreed.
The major point is that this was likely an asymptomatic finding. This was not directly relevant to his physical symptoms, but was very relevant to his LIFE! The biggest risk factor for a rupture of his abdominal aorta was the width of it. He could be smiling and talking one minute, and dead the next. That is why the complete physical is important because if someone is observant, they will likely find a concerning problem in someone.
The abdominal ultrasound found that he did, indeed, have an abdominal aortic aneurysm (dilated, compromised aorta). One that did not need surgery currently (just over 5cm….but very likely in his lifetime would need a repair). This needed to be closely monitored from now on.
I knew the classic finding I found would likely lead to this diagnosis before imaging. If you don’t know what you are looking for, you will never find it! To get an ultrasound in the first place, you have to know what you are looking for. It is a shame that medicine has become a time factor now days. I wish we could spend an hour with every patient to be very thorough…but that is not reality. There is a shortage of doctors, and we must do the best we can with the time we have.
I was happy to know that I may have found something at the right time in this guy that could prolong his quantity and quality of life. One more exam was all it took to find something serious. Artificial intelligence would not have found this because his symptoms did not correlate with this physical exam finding. It took a human and patience to find this! It makes every hard/frustrating day in the hospital turn into something meaningful. I am damn proud I found this, just as I am proud to soon become a doctor. I didn’t even tell the patient I found it. It was my job as a student to be observant, and I am just glad I didn’t let him down.
Elements of the Physical Exam:
I will highlight a few physical exam elements below. I just want to show the reader how complicated the exam can be.
I could tell many stories already in just about a year and a half of working in hospitals with the very sick, but I want to also give a glimpse at what the physical exam entails…
General:
While this may seem easy, it actually takes lots of skill, and may be one of the most important parts of the physical exam. The general exam is essentially objectifying the patient by just observation…before your tools and hands examen the patient. Are they giving you eye contact? Are they in distress? Do they look “sick.”? How much pain do they look like they are in?
This is the part of the exam where I also think about psych….What is their mood like? What is their affect like? What is their thought process?….The psych examination is mostly a “hands off” approach and many posts could be given on the psych exam— “The Mental Status Exam.”
HEENT: Head, Ears, Eyes, Nose and Throat:
This exam is a classic for children, but a a full exam should include this. It could help you find infections, cancer, vascular, and neuralgic findings.
Neurologic:

This exam when done a lot can be easily done in a few minutes or less but contains so many elements. For instance, when I do a neurologic exam I at least do a mental status (are they alert and oriented to person, place, and time?), most cranial nerves (often smell is not tested but this would include pupil size, reactivity, and accommodation... eye movement, fascial muscles, tongue movements, swallow reflex, head and shoulder movement, hearing, and so on. Then testing the sensation... (vibratory, temperature, crude touch) of whole body and face, and muscle strength. Reflexes are then often tested. One should not forget to also test functioning of the cerebellum such as heel to chin, and the dorsal columns such as the Romberg test. There are many more, and I am just scratching the surface with these. To put it plainly, it takes a lot of practice to do this in a timely but complete manner.
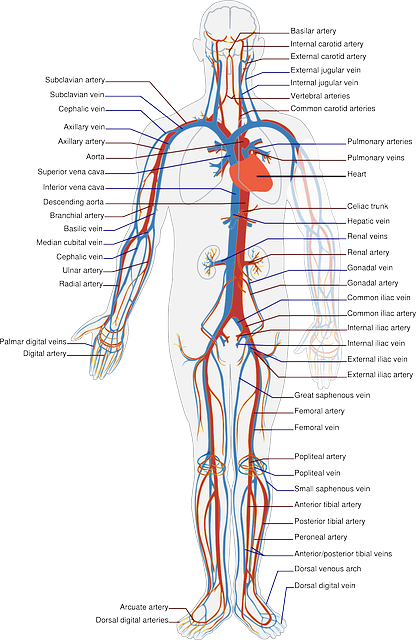
Heart/Vascular:
Is the heart beating at a regular rhythm and rate? Are there murmurs heard with the stethoscope? If so, is it at the aortic, pulmonic, tricuspid, or mitral areas? When you find the murmur loudest at a certain area, is it occurring during the systolic or diastolic phase? What is the quality of the murmur?
For example, a person complaining of a syncope episode may have a valve problem in the heart. If I heard a loud systolic murmur at the aortic area that radiated to the carotids, I would consider this to likely be an aortic stenosis. If it was in an older individual, I would assume it was due to calcifications. If it was a younger to middle age individual, I would assume it would be due to a bicuspid valve. I would get an echo, and determine the severity of this valvular problem. If it was severe, I would then believe that this could be a likely cause of a patient passing out because the brain may not be getting enough blood flow. Again, one finding...piecing together a likely etiology of the patient’s symptom. There are many more things to look for during cardiac examination, but I want you to keep reading, so I will move on.
Vascular— check the pulses…are they perfusing well? check the carotids…do they have vascular disease potentially increasing their chance of stroke and syncope?
Lungs:
Edit: Had a couple broken links above picture, which I have taken off. Thanks @justtryme90 for spotting this!
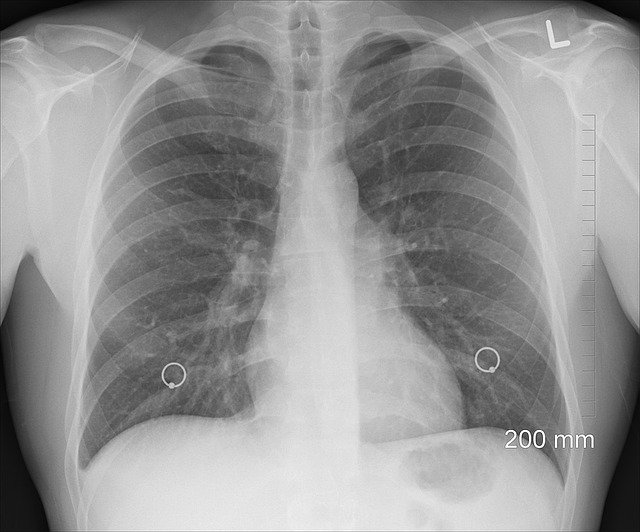
Many sounds can be heard with the stethoscope here. For example, if one has trouble breathing and is a smoker…one might hear wheezing. This could be COPD. A kid may have similar sounds...probably asthma. An important example because putting the clinical scenario into the physical exam is equally as important…Obviously, you will suspect different things. If someone has a fever and SOB and I hear crackles (rales), I would be suspecting pneumonia. Time for a chest radiograph!
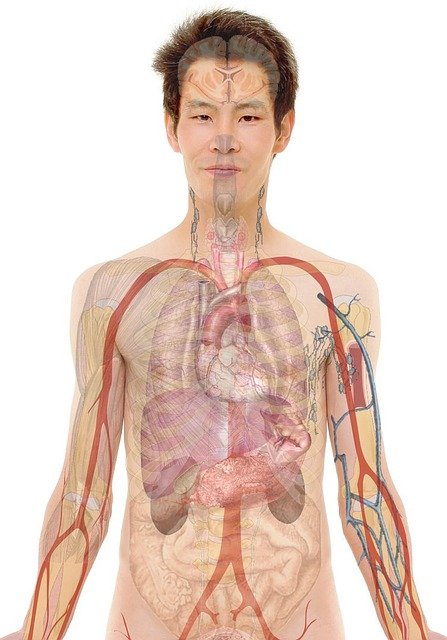
Abdominal:
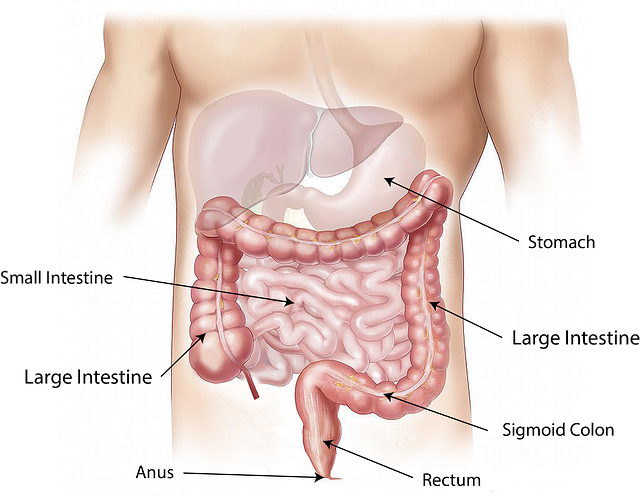
A MEGA exam…
Why?... Because there are lots of organs in your abdomen! If someone complains of upper epigastric pain, it could be the esophagus (GERD), stomach (ulcer), gall bladder, pancreas, spleen, liver, or even the bowel. To keep this part short, a great general way to think of the abdomen is if it is “acute” or not. A person in pain may be moving and showing lots of pain, but if the abdomen is soft, it is less likely to be urgent (although there are many exceptions). If someone has a rigid, firm abdomen and is in such bad pain that one is scared to move, this makes me think of the acute “abdomen.”
A later-stage appendicitis may look something like this. Peritoneal inflammation causes involuntary muscle contraction of the abdominal wall muscles. An example of the classic “appendicitis” would be periumbilical pain that then moves to terrible pain in the lower right quadrant of the abdomen. The patient may not want to move, may feel like vomiting at the thought of food, and may jump in pain if you press in the lower right hand quadrant (McBurney’s point). Also, you may elicit pain in the patient by pressing on the left side of the abdomen and quickly letting go…the patient can experience the pain again in the right lower quadrant…this is called "rebound tenderness” due to peritoneal inflammation.
There are many components to the abdominal examination such as looking, listening with a stethoscope, palpating, percussing (outlining organs by hearing the difference in sound quality by placing one hand on the abdomen while tapping with the a finger of the other hand), and special tests (like McBurney’s point).
There are also extremity exams, back, hip, and many more!
I hope this post helped show the multiple abilities needed to not only perform a good physical examination, but also to help support a diagnosis by using the patient’s risk factors and subjective history. Medical knowledge is one that takes much studying, but training to be a doctor takes so many other skills.
The detective element of being a doctor is one of my favorite aspects. It is an art. The more I learn, the less I know…but the more I want to know.
Thank you for reading, feel free to follow and comment.
*Sources: No particular source was used…just my knowledge I have gained from thousands of sources during my medical training, and from my own personal observations. Many of these tests I discussed have different sensitivities and specificities in diagnosing different diseases. The exact numbers for these were not the point of the article. The point of the article was to show the art of this element of medicine, the ability it has to save lives, and the complexity of examination that can be done rather quickly but cover so much!
*All pictures are from pixabay.com and no sources are needed
Thank you!
Me!
Read through in more detail!
Great post. One of your images (the one above the lungs) is not displaying properly.
You have given me more of an appreciation for what is going through a physicians mind when they are pushing on various parts of you during a physical examination. Thanks for this!
Thanks appreciate it!
I am glad you now understand what they are doing haha. It might seem weird but it is very important. An extra 5 minutes to listen, observe, and use hands is an essential practice.
Thanks for finding my picture issue I will fix this an soon as I am near a computer!
Outstanding post!
As I told you or @imaxess (I don't remember exactly which of you), a lot of doctors, at least in France, know in advance what you have and do not listen. It becomes very difficult to find a good family physician which really listen to the patients.
As a result, I am personally only visiting the doctor when mandatory (like for practicing sports, vaccines or under employer's demand). I am alsk very rarely sick (or I don't care and est gently for a couple of days).
That is one problem that I am glad you pointed out. I am going into family medicine as our family has for two generations before me. Specialties are very important but a different skill. The skill of trying to remember all medical conditions is hard and overwhelming. However, it is very interesting. I prefer to try and remember the essentials of everything because I believe it is important to save lives/improve quality/preventative medicine. People need family doctors to diagnose, maintain health and coordinate care elsewhere if more concentration in one area is needed. Family medicine is a specialty, a three-year program after medical school. General medicine is not easier, it's a different skill to organize hundreds of thousands of facts. Many actually find this frustrating and harder than working in one area intensely.
Thanks for the precision. You mentioned prevention! That is also something incredibly missing those days. My impression is that the society prefers to cure ill people than to prevent the from getting ill. But maybe is this a to crude generalization?
PS: if you have some time, do not hesitate to pass by the #steemSTEM channel. We would be glad to have you there :)
Treating the patient not just the disease itself is a foundational point. However, in practice it is a hard thing to do. When people have health issues, it takes time to manage this and prevention is something that is very important to try and include as well. Patient compliance is even a harder task.
Thank you for showing me this group I will check it out soon!
Fascinating glimpse into your world. It sounds like you're going to be a great doctor.
Thank you! I'm glad you enjoyed the read. It's a long journey, but one well worth it!