Rhinovirus (Common Cold Virus): Common but deadly, Understand the Virus behind the Common Cold Illness
Waking up this morning, I was severely affected by the ‘common cold’ illness (indeed it is common). Although I do know few things about it like many of us, I made some discoveries on the factors responsible for it while engaging in in-depth research.

 Common cold Patient from flickr.com
Common cold Patient from flickr.com
The common cold is a mild case of the flu disease. Although less severe and acute, it is responsible for significant unwholesomeness in humans. It is the leading cause of many students and staff missing school and the workplace respectively. But that’s not all. In the U.S.A. alone, the economic cost (cost during medical visits) regarding this illness increases at the rate of 60 billion per year[1], so you see how this affects you and your income. Perhaps try calculating how much you’ve spent treating yourself against this illness. You do know it is a viral disease, a disease caused by a virus. About 200 different viruses are responsible for the common cold, but amidst them is a king called the Rhinovirus. It is responsible for 50% of the lower respiratory infections, majorly the common cold.[2].
This post will focus on describing RHV, how we get RHV, how our body fights them and a bit of what they can do.
The King-Rhinovirus
Rhinoviruses (from the Greek word 'rhino’ which means nose) were first isolated from the mucus washed from the nasal cavity (nasal washing) of a cell biologist who was infected with upper respiratory infections in 1953 in a bid to understand the causes of the common cold. Success on their isolation was recorded more in the 1960’s due to the new culture methods which can mimic the conditions of the nose.[3]
At first, they were taught to be limited to the upper respiratory tract and its infections like the common cold that many of us get. But several studies have established their dangerous effects on the lower respiratory tract. They are associated with exacerbations (worsening/complications) of asthma in school-aged children (60-70%), cystic fibrosis in children, chronic obstructive pulmonary diseases, and chronic bronchitis in adults. They are capable of predisposing humans to other bacterial infections.[4] It has also been identified as a cause of pneumonia with severe effects in immunocompromised adults.
These entire discoveries were made more accessible by the PCR methods. Presently, there are over 160 types of this virus.They are classified into three Rhinovirus A, B, and C. Rhinovirus C was recently discovered as it does not grow in culture media and is the most dangerous of all the three due to its severe effects on humans.[5] Currently, there is no cure for the virus with most of the proposed antiviral drugs due to their toxicities, adverse interaction with other drugs, and having no effect under natural settings.[4]
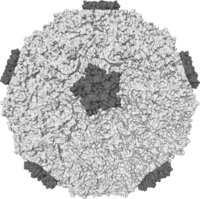
What does this deadly stuff look like?
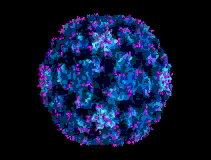
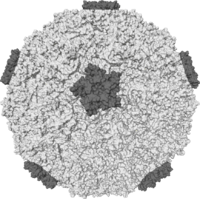
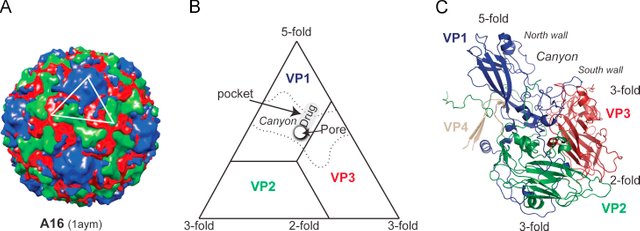
Rhinoviruses are viruses from the family Picornaviridae and genus Enterovirus. They are spherical in shape and small (≈30nm). Like every other virus, they possess a genetic material, RNA in this case, in their genome with approximately 7200 base pairs. The RNA is a special one called the positive-sense single-stranded RNA, as the RNA sequence can be easily translated into proteins. The viral genome undoubtedly also contains a gene which encodes viral proteases (ignore the name; they are enzymes which deal with protein) which divides the translated polyprotein to produce eleven proteins.[6]
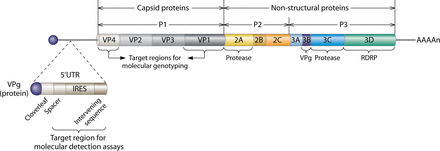
The genome is enclosed in a protective shell called the capsid which takes any shape depending on the arrangement of its structural proteins. The Rhinovirus capsid is made up of four structural proteins (VP1, VP2, VP3, and VP4), with the smallest, VP4, holding the RNA core to the capsid, and VP1-VP3 responsible for the difference in the antigenicity of rhinoviruses. The capsid is icosahedral (a type of polygon shape from our basic mathematics) in form due to the presence of 60 copies of each of the four viral proteins. The VP1-VP3 are structurally similar with their C termini (carboxyl group ending the protein) and N termini (amine group at the starting point of the protein) located on the internal and external surface of the virion respectively. The genome also contains non-structural proteins which are involved in its replication and protein processing.[4]
Some viruses (Coronavirus and the Hepatitis D virus) also include an envelope, a protective lipid layer on the capsid (trying every method to protect themselves). This envelope helps them enter into the host but is sensitive to detergents and heat, and thus are easy to kill or deactivate. No, rhinoviruses are just stubborn as they lack this envelope which makes them resistant to fluorocarbons, ether, and chloroform.[7]
They are lovers of cold temperatures so can persist for years. They infect best at 24-370C which makes them survive for hours to days on surfaces in our homes like cups and door handles, and for two hours on our skin undisturbed. Some of them can also remain unchanged at higher temperatures (e.g., 500C), but this behaviour varies among the stereotypes.[8]
Majorly, the structural differences between the stereotypes occur on the loops of the external surfaces of the capsid joining the B strands and on the internal surfaces of the capsid, the N termini—particularly that of VP4 and VP1. For instance, in the HRV3 and HRV14, the N terminal ends are disarranged while in HRV1A, it is the VP4 alone. They are similar to Enterovirus based on their evolutionary history (genus) but different by behaviour in an acidic environment as they can only withstand PH values from 6.0-8.0 and rendered inactive at PH values below 6.0.[9]
How they replicate (reproduce) inside of you and for how long
Oh, this is their primary mission. Replicating is a scientific term for reproduction for viruses. And they can only do that in a living cell, so you see why they love you.
How do they do that?
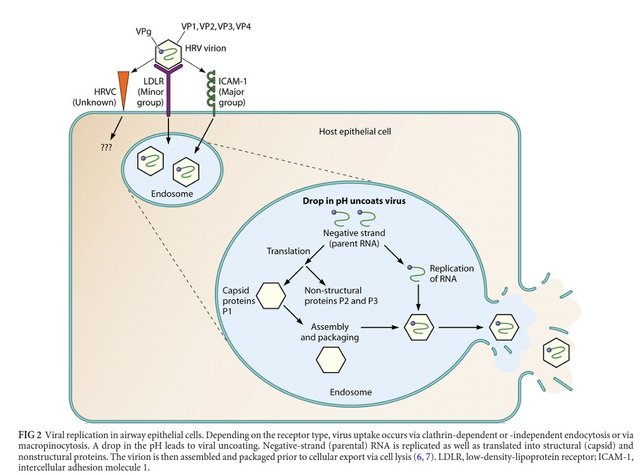
First, they attach themselves to our nose’s epithelial cells using receptors present on the cell surface. The receptors are kind of cellular glycoproteins that signal to the cell that an extracellular molecule (hormone or nutrients) is on its way into the cell. The receptors utilized by RV could either be an intercellular adhesion molecule 1 (ICAM-1), or low-density lipoprotein (LDL) receptors, or the recently identified cadherin-related family member 3 (CDHR3) receptor. The ICAM-1 is mostly employed by Rhinovirus A and B (major group), and the LDL receptor is used by twelve types of Rhinovirus A species (minor group).[4] The CDHR3 receptor is used by the RV C although little information exists on its function and mode of interaction with Rhinovirus C due it just being discovered.
Process of reproduction reproduce from [1]
Once they get attached to the receptors, they change (a conformational type) in their capsid to release their viral RNA into the cell cytoplasm via endocytosis (which might be clathrin-dependent or independent in the case of HRV2 and HRV14 respectively).[4] Endocytosis is merely the process by which one cell in our body transports molecules into another cell by engulfing it, and clathrin is a protein that aids endocytosis by forming coated vesicles in the cytoplasm. An example of endocytosis is how cells in our body receive cholesterol and iron into their cytoplasm, a part of the cell where most of its activities take place. So RV hijacked this process to get into our cells’ cytoplasm.
The virus RNA is translated into a long polyprotein, a kind of protein that yields polypeptides (a combination of many amino acids) by the ribosome in the cytoplasm. The polyprotein divides to form proteins, a process called cleaving. The polyprotein cleaves with the aid of two proteinases (2A and 3C/3CD) to create three intermediates proteins (P1, P2, and P3). P1 divides to form VP1, VP3, and VP0 which also cleaves to produce VP2 and VP4 during assembly of the capsid (LOL, they do like splitting). As earlier stated, the VP’s are the structural proteins of the RV, the new virus in this case. Other proteins that are created include RNA-dependent RNA polymerase, protease, and VPg; all produced from P2 and P3.[10,11]
This process of replicating themselves took up to 10-12 hours in an in-vitro experiment (cell culture) although they were detected as early as seven hours. However, in a test where adult volunteers were challenged with HRV39, rhinoviruses were recovered at 11.3 ( range=8-18) hours in nasal washings of the adults; highest titer value of the virus was discovered at 48 hours, but later declined at the third day to the fifth day.[7,12]
But how do you get it? (Transmission)

We either get it from other people through contact (direct or fomite-infected objects), or air droplets (aerosols). Its infection is kicked off by inoculating the nose or eye (goes through the lacrimal duct which connects the eye to the nose) with the virus.[13] Inoculation merely is the introduction of some substance or organism into the body, majorly through vaccines. Attempts to inoculate the mouth with the virus have not been efficient or let’s say, failed. Under experiments settings, they are placed on the hand and released into the environment. Our nose mucosa temperature is similar to their optimal growth temperature (330C) which explains why they love our nose.
It is easy to spread amidst families, especially when a member of the family is infected, particularly children. Twenty-four couples, of which one of the partners was infected with the virus (experimentally), were studied under contact periods varying between 63 to 149 hours, and nine of them were discovered to have acquired the infection.[14] In another study using aerosols, 56% of the 18 card players were infected after playing with infected players for 12 hours.[15]
Epidemiology: Distribution across the human population
Seasonal Variation: They are everywhere, anytime, all year. They yield infections and respiratory illness during the whole of a year, and its entire species are spread evenly throughout the world.[16] It has been discovered that there is always a high peak of RV infections in early autumn and a smaller peak in spring for the temperate climates. Surprisingly, the top height in autumn is in harmony with the start of the school year, which explains why children are the most affected (poor kids).[17] However, the same explanation cannot be used for the spring peak. During the autumn, 80% of the common cold illness is caused by RV, athough they are not the only viruses involved with the common cold illness. Although respiratory infections are low in the summer, on isolating, RV accounts for the primary cause of the disease.
For the tropical climates, high respiratory infections have been observed at the opening and closing of the rainy season.[17] An explanation for this seasonal variation exhibited by RV’s has not been established yet, although their ability to survive in an environment with RH greater than 50% has been proposed as one of the reasons for the variation.
Age-influenced variation: Children have been established to be the frequent victims of rhinovirus infections in numerous studies. It occurs so early that at six months of age, 20% of children have tested positive for RV in their serum, and so sad that at two years of age, 86% of children had encountered one RV infection or the other.[18] RV accounts for 73% of total acute respiratory infections tested so far in children as shown in the table. The relationship between the rate of infection and age is an inverse type with the age group (20-29) being exempted.[19]; increased exposure of parents to children at this age was considered as the cause for the exemption which seems too reasonable to be true. Although, I fall within that age group; I am not always with my parents. RV's are however not limited to children, as high incidence of RV infections has been noticed in adults of 60 years and older using RT-PCR.[20]
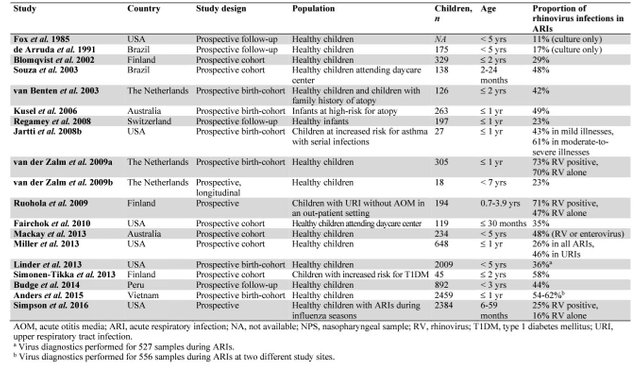
Several studies on rhinovirus infections in acute respiratory infection reproduced from [29]
How our body fights. RHV
Innate immune response: The first line of defense in our body against rhinovirus infections are the cells of the epithelial airway as they secrete enzymes or peptides like lysozyme and cathelicidin which perform an antimicrobial activity. The sneezing and cough we experienced are part of the mechanism of getting rid of these pathogen’s viruses.
Our body identifies and response to rhinovirus on getting infected with them quickly. How?
The epithelial cells in the nose possess types of receptor called the pattern-recognition receptors which act as sensors or send signals to the immune systems. On recognizing specific molecules (known as the pathogen-associated molecular patterns), embedded within microbes different from cellular molecules, they send a message to the innate immune system which activates the immune response to the virus.
Rhinoviruses are recognized by two pattern-recognition receptor families: TLRs and retinoic acid-inducible gene-I-like receptors (RLR), an RNA helicase family that includes retinoic acid-inducible gene-I (RIG-I), melanoma differentiation-associated gene-5 (MDA-5), and LGP-2 (laboratory of genetics and physiology 2).[4,11]
On internalization of the virus genome (i.e., upon entering into the host cell), dsRNA is recognized by TLR3 while ssRNA is identified by TLR7 and TLR8 situated in the endosome of the host cell. Toll-like receptors (TLR) are protein receptors that got their name from the toll protein of the fruit-fly (Drosophila). TLR2 recognize the virus capsid at the surface of the host cell which induces production of cytokines using MyD88-dependent pathway. Once new ssRNA and dsRNA are synthesized, they are identified by RIG-1 and MDA-5 in the cytoplasm which instigates the expression IFN gene and increases production of neutrophil cytokines such as interleukin (IL)-8 and others as shown in the image. These cytokines attach themselves to receptors of neighboring cells to release proteins which have anti-viral properties.[21,22]
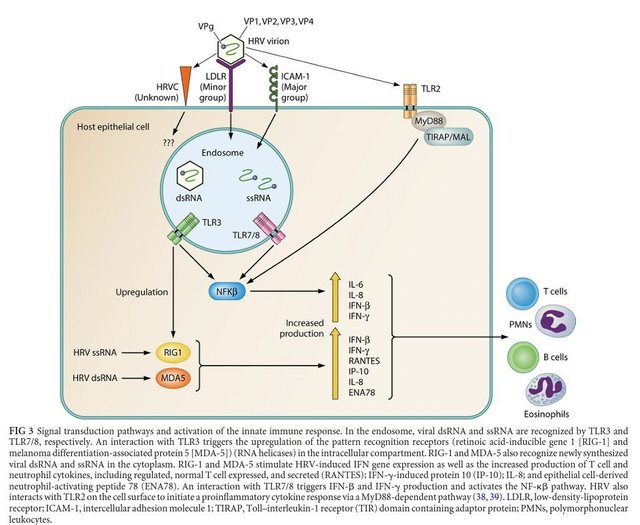
The Signal Transduction Pathway:How our immune system fights HRV,reproduced from [1]
Adaptive immune response: This type of response is activated together with the innate immune response, but slower. It was discovered that RV enables the production of nasal secretory IgA antibodies, serum type-specific neutralizing immunoglobulin (Ig) G antibodies, and specific T-cell response. These antibodies are noticeable at one to two weeks in an experimental setting and remain high for years.
A high level of serotype-specific antibodies confers protection from infection and is associated with milder symptoms after experimental infection with the same serotype (immune-memory: the antibodies have a memory of the first virus infection so they act faster towards the second infection thus yielding less severe symptoms). Little cross-neutralization exists amidst the stereotypes which are the primary hindrance to vaccine development due to the presence of many HRV stereotypes.[23]
T-cells also play a role in immunity against RV by recognizing the virus antigens, thus inducing antibody-mediated immune responses and production of cytotoxic, i.e., the immune cells act as toxins to the virus cells, now killing or deactivating them. The Secreted RANTES and IP-10 of our innate immune system aid T-cell chemotaxis[24](i.e., movement in response to the chemical signals send by the receptors to destroy the virus).
Clinical Presentation
Common cold: This illness is a mild one and usually self-limiting, i.e., would resolve itself without an external agent or treatment. Rhinovirus causing common colds have a shorter incubation period—8-10 hours under experimental settings and an average of two hours in immunocompetent humans (people capable of inducing an immune response because not all humans can instigate the immune response like the HIV infection, i.e., immunodeficient.[25] The first symptoms are displayed soon after infection and attain a peak between the 2nd and 3rd day of infection. Sore throats are usually the first symptom (but not in all cases), with sneezing, nasal congestion, cough, malaise, nasal obstruction, rhinorrhea, fever, and headache following. On average, the symptoms can last for seven days in youths and up to two weeks in one out of four cases in old ones and children.[26]
More deadly actions
Acute otitis media (AOM): This is one of the results of the complication of rhinovirus infections particularly in children at the beginning of common cold symptoms within the first week. Symptoms revealed in volunteers who were inoculated with HV through the nose include Eustachian tube dysfunction, abnormal middle ear pressure which contributes to the development of acute otitis media. Further confirming this was research on the adenoid tissue (tissue behind the nasal cavity) of children suffering from persistent OM of which 45% had RV RNA on their adenoid tissue. ).[27]

Rhinosinusitis: This is the inflammation of the air-filled spaces (paranasal sinuses) surrounding the nasal cavity. The paranasal sinuses are often affected by RV infections in the early days of the common cold leading to sinusitis/Rhinosinusitis and usually rectified without any treatment. Confirming this natural rectification was a study by Gwaltney who discovered that 87% of the patients with the common cold possessed the abnormalities in their maxillary sinuses, and 79% of the patients’ defects were resolved without using antibiotics in two weeks. ). These sinus abnormalities are usually detected using computed tomography or magnetic resonance imaging in patients with the common cold.[28]
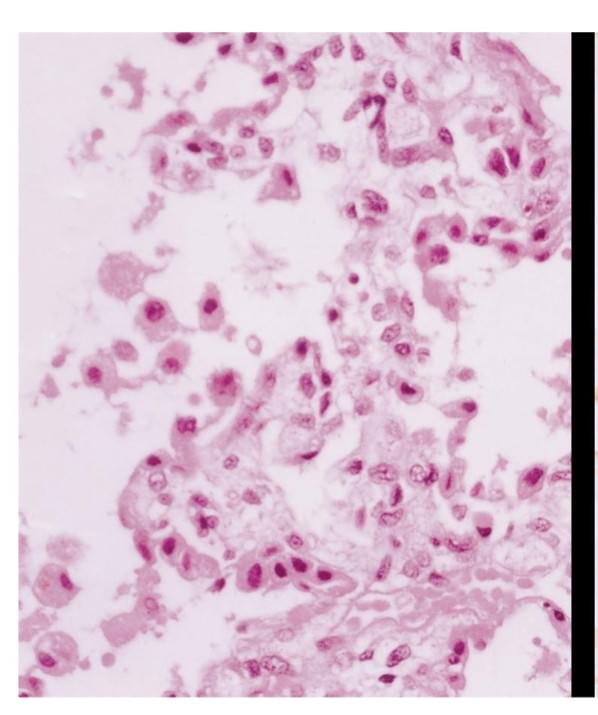
These are not all of their destructive actions; the rest will be discussed in the next post. But I will leave you with this picture of the lung tissue of an infant who died as a result of pneumonia due to rhinovirus.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
REFERENCES
[7] Stott, E. J. & Killington, R. A. (1972). Rhinoviruses. Annu Rev Microbiol 26, 503-24.
[10*] EPIDEMIOLOGY OF HUMAN RHINOVIRUSES by Soile Blomqvist , (2004).
[11] Racaniello, V. R. 2001. Picornaviridae: the viruses and their replication, p. 685-722. In D. M. Knipe and P. M. Howley (ed.), Fields virology, 4th ed., vol. 1. Lippincott/The Williams & Wilkins Co., Philadelphia.
All pictures are sourced within the post. References with * are the major ones, so could read them to understand more. RHV:RHINOVIRUS AND TLR:TOLL LIKE RECEPTOR
If you are interested in writing science post or like reading scientific posts, could join the SteemSTEM community. A community devoted to understand and making science know to people. Join us on steemitchat through the SteemSTEM channel or on discord.

Thanks to @rocking-dave for the gif.
Nic post
some of those pics are pretty gross !
what really this happens i take very lightly but its really harmful thanxs sir for awaring the generation of this deadly virus thanxs alot
very nice and useful post, good work friend
Thanks for the information
thanks for this.
insightful...I learnt a thing or two...kudos
So Rhino virus is responsible for the condition I'm experiencing now,
Hmm i wish they were big enough so i could squash them!
LOL
Definitely bro
That's even if they are visible to your eyes
Sorry anyway
Just rest though is self limiting
No problem sir