Paediatrics #1 - What is Lumbar Puncture?
Lumbar puncture is one of the few diagnostic tools for neurologist. In comparison to the wicked craniotomy, the spinal tap (or lumbar puncture) has way better reputation as they reported only seldom severe side effects. This procedure has several scientists to thank for its great life-saving investigation technique.
History of Lumbar Puncture
In the fourth century, Hippocrates was the first person to hint at the very existence of the CSF or the cerebrospinal fluid. He was first to found out the existence of ventricles in the brain, the container of all the CSF. He was however failed to relate the correlation between ventricles and CSF (as he called it water in the brain) at that time. Galen, another scientist, found that clear fluid are present in the brain as he was dissecting several animals. Not until 1692, an Italian anatomist Antonio Mara Vasalva took note of a clear liquid after dissecting though a dog’s spine. He was a researcher that is well known to taste human exudates but interestingly there was no documentation regarding the taste of CSF by him. He has tasted far more unpalatable samples like the gangrenous ooze before, yikes..
His disciple, Domenico Cotugno finally discovered the subarachnoid CSF in human in 1764. About 90 years after that, Faivre managed to pinpoint the exact source of CSF, which is the choroid plexus. The technique of accessing the dural space was first described by the London physician Walter Essex Wynter. He was inspired by the relative success after inserting drainage tubes to treat severe edema (swelling) in the limbs back in the Victorian age and thus, he applied the same concept to treat “brain swelling”. This type of lumbar puncture was aimed to reduce the intracranial pressure instead of diagnostic purposes. Few cases were partially treated by Wynter as in February 1889, he made a small midline incision at the second lumbar vertebrae and inserted a thin cannula fitted with a rubber tube into the dura in order to drain the fluid. Yes, the procedure provided somewhat a temporary relief but the patient died due to meningitis (inflammation of the meninges lining in the brain) possibly caused by an ear infection.

The real man that actually managed to figure out the properties of the cerebrospinal fluid is none other than the Frankfurt-born Heinrich Irenaeus Quincke. He graduated from the University of Berlin and became a shining star in Surgery and Internal Medicine. In the year of 1872, he ingeniously coloured the CSF of dogs with the colour red by introducing the sulphide mercury in the subarachnoid space so he could trace the flow. In 1888, Quincke subjected a 12-year old boy to several CSF drainings from the cerebral ventricles using a cylindrical blade through punctured holes in his skull. Well, the boy died after the procedure, which is hardly a surprise. In dismay, Quincke further refined his technique and successfully performed the very first lumbar puncture on a 21 months old boy. He used a thinner cannula injected between the third and the fourth lumbar vertebrae. He managed to withdraw CSF three times over three-day interval and the boy survived!
During his Lumbar Punctures, Quincke paid full attention to the fluid pressure (which is known as the opening pressure) and tested for glucose and protein levels within the fluid. He was then pretty much interested in making lumbar puncture as a diagnostic tool and he proved his point after he found tubercle bacilli in the CSF of affected patients. It is then known as the “Quicke’s Puncture”. Anesthesiologists soon develop effective methods of spinal anaesthesia by injecting cocaine and then better drugs after that. The pain relief technique brought by these pioneer anaesthesiologists provide tremendous improvement to the world of medicine, especially in the surgical field.
CSF or Cerebrospinal Fluid
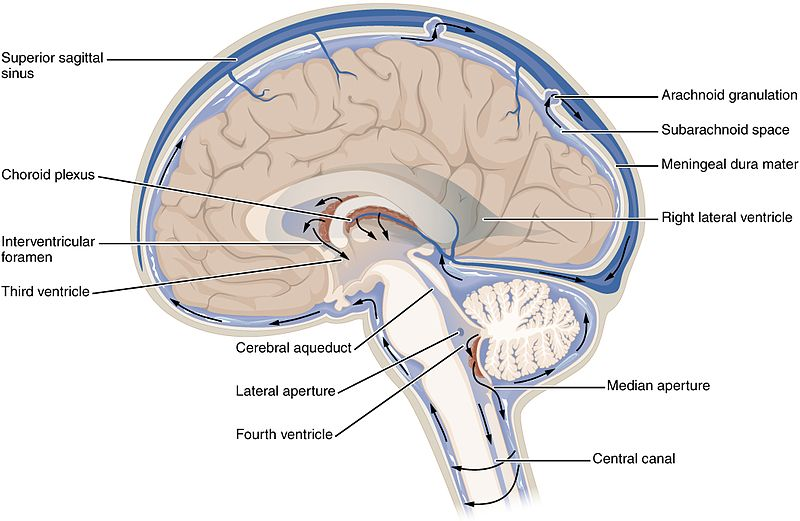
The brain and spinal cord are coated with layers of cerebrospinal fluid with about 125-150ml in total. It acts as a shock absorber, a medium to transfer nutrients and waste product, prevention of brain ischaemia by reducing the total CSF volume in the brain to allow more blood perfusion, regulation of endocrine factors, and maintain the buoyancy of the brain.
500ml of CFS are produced daily by the brain, at around 25 mL per hour. Approximately 80% of the CSF produced comes from the choroid plexus. They are network of blood vessels which are scattered within the four ventricular walls of the brain. The remaining unused CSFs are reabsorbed back into the system via the dural venous sinuses. They contain valves that only permit one way drainage. Furthermore, some of the CSFs are drained into the lymphatic system, particularly those nearby the nasal region, along the olfactory nerve. Hence that’s why if there’s any injury or trauma at the nose, it can leak CSFs.
What does CSF made of?
They originate from blood plasma with the exception that CSFs are protein-free. CSF has a higher chloride level but with similar sodium level, as compared to the blood. Typically, CSFs are free from hemoglobins with little white blood cells. Presence of blood or excessive white cell count (which is known as pleocytosis) in the CSF might point out to some diagnoses.
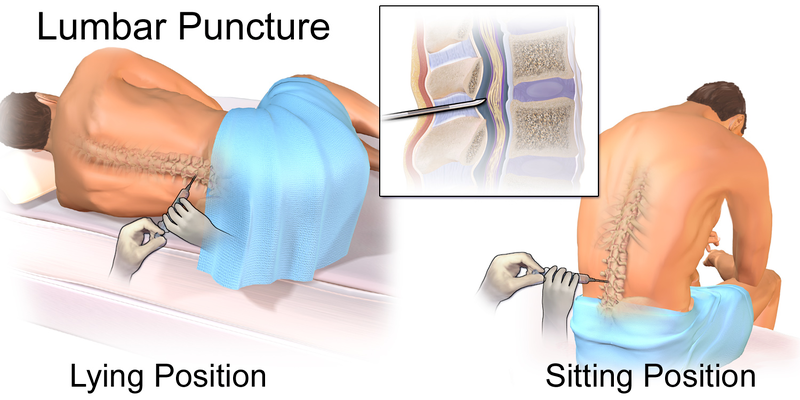
Technique of obtaining CSF

CSFs can be obtained via puncturing at the lumbar cisterns, usually below the first or second lumbar vertebrae. This is where the spinal cord terminates, a region called the conus medullaris. Below this, nerve still continues but in a loose, fan-shaped fibers called the cauda equina. Hence, it is recommended to insert the needle at the cauda equina region, to avoid puncturing the spinal cord (which can cause paralysis).
Interpretation of CSF
1) CSF Pressure
The CSF opening pressure is around 8-15mmHg (lying) or 16-24mmHg (sitting up). Increased in CSF opening pressure can be related to conditions such as congestive cardiac failure, subarachnoid hemorrhage, cerebral edema, inflammation of the meninges, hydrocephalus, and idiopathic intracranial hypertension.
2) Cell count
As I’ve mentioned earlier, an increase in white cell count in the CSF is termed as Pleocytosis. Conditions those could give rise to this problem are meningitis, leukemia, central nervous system hemorrhage, or tumours.
3) Microbiology
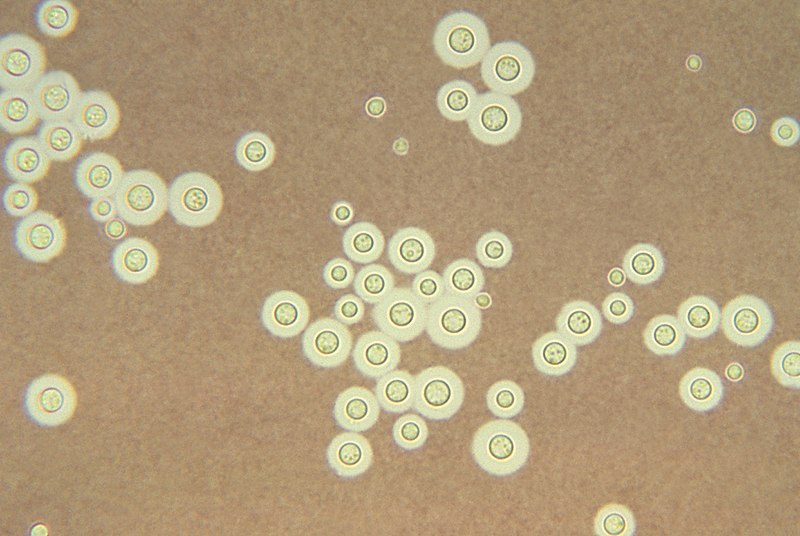
CSFs should be sent to the microbiology lab to determine the causative agent especially when meningitis or encephalitis is suspected. Gram staining of the fluid can be done to differentiate whether the organism is gram positive or gram negative. Various microbiological cultures can be inoculated from CSFs to multiply the organism, further aiding in diagnosis. The india ink test or the cryptococcal antigen (CrAg) can be done to isolate Cryptococcus neoformans as a causative agent of meningitis, especially in those with poor immune system.
4) Chemistry
The glucose level of the cerebrospinal fluid should be measured especially to differentiate the causative agent of meningitis; viral or bacterial. In normal situation, the glucose level in the CSF is about 60% from the blood glucose level. If the value is lesser than 60%; bacterial, fungal or even tuberculous causes are more likely than viral. Furthermore, CSF lactate dehydrogenase can be measured as bacterial infection usually result in higher level of the enzyme as compared to viral causes.
Contraindications of lumbar puncture?
One of the most gruesome situation that can result from lumbar puncture is cerebral herniation, specifically the uncal herniation. Herniation means a condition that arises when the organ is displaced and protrudes through the wall of cavity containing it. This is especially true when there’s a cerebral mass causing an increase in intracranial pressure. Confused already? Okay. Imagine that there’s a pathway that connects the CSF in the brain and the CSF in the spinal cord. When there’s a cerebral mass that occludes the pathway, there will be increase in intracranial pressure due to the mass itself. Signs of raised intracranial pressure such as focal neurological deficits, reduce conscious level and bulging of the optic disc on funduscopy examination (papilloedema).

If we still proceed with a lumbar puncture, the CSF escape causes low pressure outlet at the spinal cord region because of the obstructing intracranial mass. It’s like when you pinch a vertical tube in the center when there’s water on the upper part of the tube. This low pressure outlet causes uncal or transtentorial herniation. As in the brain matter or mass will displace towards the low pressure area (known as the brain shift) causing significant amount of catastrophe to the individual because that part of the brain controls many functions of the body. Hence, CT scan is recommended prior to lumbar puncture especially those with signs of raised intracranial pressure to avoid horrifying complications. Other relative contraindications include coagulopathy because excessive bleeding can occur after puncturing.
In conclusion, lumbar puncture and the analysis of cerebrospinal fluid has been a part of the medical field for over one hundred years. The procedure is very simple and yet poorly educated physicians might end up causing more harm than good if the knowledge regarding lumbar puncture is inadequate. Lumbar puncture is a life-saving procedure and the diagnosis of meningitis can prevent a lot of morbidities to the patients. With that, thank you :)
References
- Rosenhek J. Point Well Taken. Doctor's Review. Retrieved on May 26, 2018 from http://www.doctorsreview.com/history/point-well-taken/
- Lumbar puncture - Technique, indications, contraindications, and complications in adults. Retrieved on May 27, 2018, from https://www.uptodate.com/contents/lumbar-puncture-technique-indications-contraindications-and-complications-in-adults
- Lumbar Puncture. School of Medicine, Queen's University. Retrieved on May 26, 2018 from https://meds.queensu.ca/central/assets/modules/lumbar_puncture/introduction.html
- Lumbar puncture and the risk of herniation: when should we first perform CT?. Journal of Neurology. Retrieved on May 27, 2018, from https://link.springer.com/article/10.1007%2FPL00007855
- Lumbar Puncture. Wikipedia. Retrieved on May 26, 2018 from https://en.wikipedia.org/wiki/Lumbar_puncture
- Cerebrospinal fluid. Wikipedia. Retrieved on May 26, 2018 from https://en.wikipedia.org/wiki/Cerebrospinal_fluid
You've been upvoted by TeamMalaysia Community :-
To support the growth of TeamMalaysia Follow our upvotes by using steemauto.com and follow trail of @myach
Vote TeamMalaysia witness bitrocker2020 using this link vote for witness